Eric Brindle BSE Student1,3 ; Dany Gagnon, PT, PhD1,2 ; Alicia Koontz, PhD, RET1,3 ; Rory A. Cooper PhD1-3 .
(1) Human Engineering Research Laboratories, VA Pittsburgh Healthcare System
(2) Department of Physical Medicine and Rehabilitation, University of Pittsburgh
(3) Department of Bioengineering, University of Pittsburgh
ABSTRACT
A wheelchair transfer test, completed by 14 participants from the preferred and non-preferred side, was designed to investigate muscular demand of seven essential shoulder and elbow muscles during sitting pivot transfers in the leading and trailing upper limb (U/L). All participants were connected to surface electromyography (EMG) to determine peak muscle demand as well as an indicator of overall muscle demand to quantify results. All EMG data were filtered with a bandpass butterworth filter then normalized to the EMGmax. The biceps brachii had a trend towards significant (p=0.053) with 6.0% higher values in the non-preferred approach and the anterior deltoid had a significant difference with 25% higher values in the trailing U/L (p=0.008). A larger sample may lead to less variability as well as more significant results.
KEY WORDS
Biomechanics, Transfers, Electromyography, Upper Extremity, Wheelchair
BACKGROUND
Individuals who sustain thoracic spinal cord injuries (SCI) generally experience severe sensory and motor impairments affecting the trunk and lower limbs. Since these impairments drastically reduce their ability to ambulate, most of these individuals will become long-term manual wheelchair users and will consequently perform sitting transfers numerous times daily1-3. Since the U/Ls are highly solicited during these functional tasks, it may increase the risk of developing secondary U/L musculoskeletal impairments over time1,2,4. Manual wheelchair propulsion has been studied extensively over the past decade whereas there is a paucity of studies focusing on sitting transfer tasks among individuals with SCI4.
The U/L risk potentially linked to sitting transfers has led to an increased interest in biomechanical and clinical assessment of this demanding task1-5. Perry et al. as well as Nyland et al. have found elevated muscular demand during transfers in the latissimus dorsi, pectoralis major, anterior deltoid, lower trapezius and triceps1,3. The high muscular demand found at the pectoralis major and the anterior deltoid has been associated to the contribution of these muscles to generate shoulder flexor and adductor moments as well as elbow extension moments as the U/Ls are recruited in a closed kinetic chain during sitting pivot transfers. These studies, however, failed to assess the muscular demand effects of transferring from both the individual’s preferred and non-preferred side. An individual is not always able to dictate the side in which they complete the transfer, for instance, when transferring into the passenger side of a vehicle.
For this reason, we quantified muscular demand during a sitting transfer between level surfaces to investigate differences in transferring from the individual’s preferred side as opposed to their non-preferred side. The objective of this study was to compare muscular demand at both U/Ls during sitting pivot transfers as well as determine if there is a muscular advantage in transferring from the preferred side as opposed to the non-preferred side during level transfers. In an attempt to explain the preference, it was hypothesized that the muscular demand for the preferred side would be less than that of the non-preferred side.
METHODS
Participants:
Fourteen (13 males; 1 female) participants with complete and incomplete thoracic spinal cord injuries (SCI) were recruited to take part in this study from the 2008 National Disabled Veterans Winter Sports Classic (Snowmass Village, CO; March 30 – April 4, 2008). On average (mean ± 1SD), participants were 47.0 ± 8.3 years of age, 1.8 ± 0.08 m, and 75.3 ± 11.3 kg with SCI levels ranging from C6 to S1 . Only participants that use a wheelchair as their main source of mobility (40+ hrs per week in wheelchair) as well as have the ability to complete sitting transfers without technical or human assistance were recruited for this study. At the time of testing, no participant complained of any sign or symptom of trunk or U/L impairment that would affect the way in which they routinely complete their transfers. All participants reviewed and signed an informed consent prior to entering the study.
EMG Data Collection:
Bilateral surface EMG was collected for the sternal and clavicular fibers of the pectoralis major, anterior deltoid, biceps brachii, triceps brachii, inferior trapezius, and the latissimus dorsi during the transfer tasks using Noraxon software (Telemyo 2400T). Small Ag-AgCl surface electrodes (Blue Sensor Electrodes, N-00-S) were placed directly over the muscle belly parallel to the orientation of the muscle fibers in a bipolar configuration. A detailed description of the electrode placement for each muscle can be seen in Table 1. A reference electrode was placed on the manubrium sternae. All electrode leads were secured to the U/L and trunk segments before being connected to one of the two NORAXON transmitting units (TeleMyo900, 0.453 kg) secured posteriorly on the waist of the participant. All signals were digitized at a sampling frequency of 1500 Hz before being sent to the MyoResearch XP Master Edition software to view and store the EMG data. An accelerometer was attached to the C7 spinous process and was synched with four pressure sensors, located underneath the buttocks, as well as a digital web cam recorder to facilitate data analyses.
| Muscle | Placement of the electrodes |
|---|---|
Pectoralis major (clavicular fibers) |
Midway between the coracoid process and the sterno-clavicular joint 2 cm below the clavicule |
Pectoralis major |
2 cm medial to the anterior axillary fold in direct vertical line with the coracoid process |
Deltoid |
2 cm distal and anterior the acromion |
Biceps brachii |
Center of the muscle belly |
Triceps brachii |
Midway between the olecranon and the acromion at 2 cm medial to the line over the muscle belly |
Trapezius |
At 2/3 on a line from the trigonum spinae to T8 spinous process |
Latissimus dorsi |
2 cm inferior and lateral to the inferior angle of the scapula |
Maximum Voluntary Contractions (MVCs):
The MVCs were performed for all muscles investigated prior to performing the transfer tasks using a standardized manual testing protocol. Participants were asked to gradually increase their muscular effort to their maximum output while the investigator supplied manual resistance with one hand and stabilized the participant’s proximal body segments with the other. The MVCs were held between 3 and 7 seconds prior to recording. These static muscle tests were necessary to determine the EMGmax of each muscle. The EMGmax was used to normalize all EMG values obtained during the transfer tasks.
Sitting Pivot Transfer Tasks:
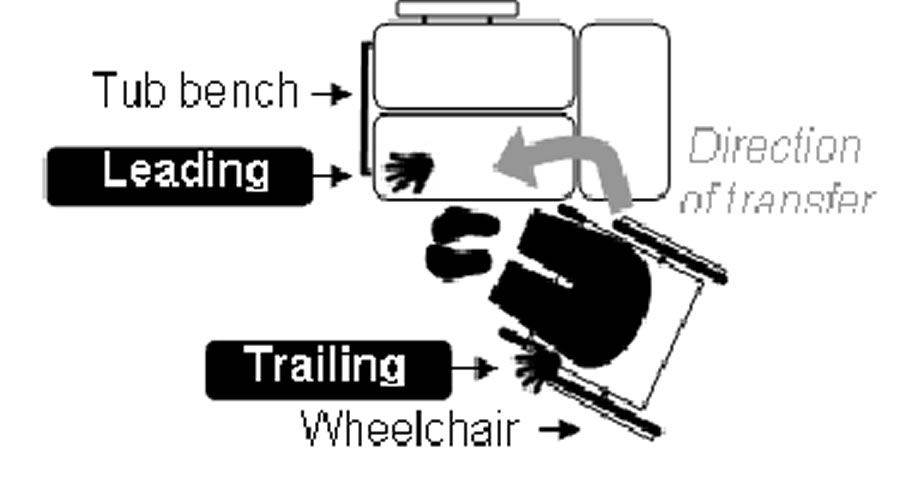
Figure 1. (Click for larger view)
Participants were instructed to transfer from their personal wheelchair to a target padded tub bench (Rubbermaid Inc.) set at a height equivalent to the combined height of the participant’s wheelchair and seat cushion. Participants completed the transfers with the trailing hand positioned on their personal wheelchair and their leading hand positioned on the target bench (Figure 1). After a familiarization period, participants were instructed to complete the transfer from the side in which they were most comfortable to determine preferred side measurements (task #1: Preferred approach) followed by completing the transfer from the opposite side to determine the non-preferred measurements (task #2: Non-preferred approach). Participants completed a total of three transfers in each direction. The initial positioning of the wheelchair (angle of wheelchair to bench) as well as the hand, feet and buttocks positions were self-selected and marked to assure similar starting positions across all trials and between the preferred and non-preferred transfer approaches for each participant. The start of each transfer corresponded to the start of acceleration captured by the accelerometer. Rest periods were also given as needed to limit the affects of fatigue.
EMG Data Analysis:
All EMG data collected were filtered using a bandpass butterworth filter with cutoffs at 30 and 500 Hz. The 30 Hz cutoff was set to remove any electrocardiographic contaminations6. Then, the EMG values were full-wave rectified before being filtered with a low-pass 6Hz filter to create linear envelopes. The EMGmax value for each muscle was determined by finding the highest mean EMG values recorded over consecutive periods of 0.5 second intervals during the MVC. The EMG values found during transfers were amplitude-normalized against the EMGmax to quantify muscular utilization ratio (MUR) (Equation 1).
Equation 1.
MUR Transfer (%) = (EMGtask /EMGmax )*100
Transfer (%) = (EMGtask /EMGmax )*100
An overall muscle demand indicator was also calculated by integrating the MUR curve found during the transfer. All data analysis was completed in a custom made Matlab program (The Mathworks, Natick, MA).
Outcome Measures:
The peak MUR as well as overall muscle demand of each muscle was used as primary outcome measures in this study. Peak MUR was considered high if the MUR value obtained exceeded 50%, moderate if it was in the range of 25 to 50% and low if below 25%2.
Statistics:
For all muscles, repeated measures analyses of variance (ANOVA) [2 approaches (preferred vs. non-preferred) × 2 U/L roles (leading vs. trailing)] were applied to determine if the transfer approach or U/L roles played a part in the muscular demand. In absence of interaction, main effects were reported whereas, in presence of interaction, paired sample t-tests were used to further investigate any significant outcomes. A level of significance of 0.05 was selected for all tests. Statistical analyses were performed using SPSS® software.
RESULTS
All participants were able to independently complete the transfer test from their preferred side as well as their non-preferred side. The biceps had a trend (0.05<p<0.1) towards significant (p=0.053) in the transfer approach with the non-preferred side having 6.06% greater peak values as seen in Table 2. Only the peak values of the anterior fibers of the deltoid were found to have a significant difference between the leading and trailing U/Ls (p=0.008) with the trailing U/L having a 25.07% greater peak muscle demand (Table 3).
| Muscle | % Difference |
p-value |
|---|---|---|
Pectoralis Major (Clavicular Fibers) |
0.38 |
0.934 |
Pectoralis Major (Sternal Fibers) |
-2.54 |
0.467 |
Anterior Deltoid |
-3.63 |
0.281 |
Biceps Brachii |
6.06 |
0.053 |
Triceps Brachii |
0.22 |
0.961 |
Inferior Trapezius |
-1.3 |
0.527 |
Latissimus Dorsi |
13.5 |
0.212 |
Muscle |
% Difference |
p-value |
Pectoralis Major (Clavicular Fibers) |
5.03 |
0.572 |
Pectoralis Major (Sternal Fibers) |
9.14 |
0.125 |
Anterior Deltoid |
-25.07 |
0.008 |
Biceps Brachii |
2.12 |
0.838 |
Triceps Brachii |
19.69 |
0.203 |
Inferior Trapezius |
4.18 |
0.538 |
Latissimus Dorsi |
8.6 |
0.214 |
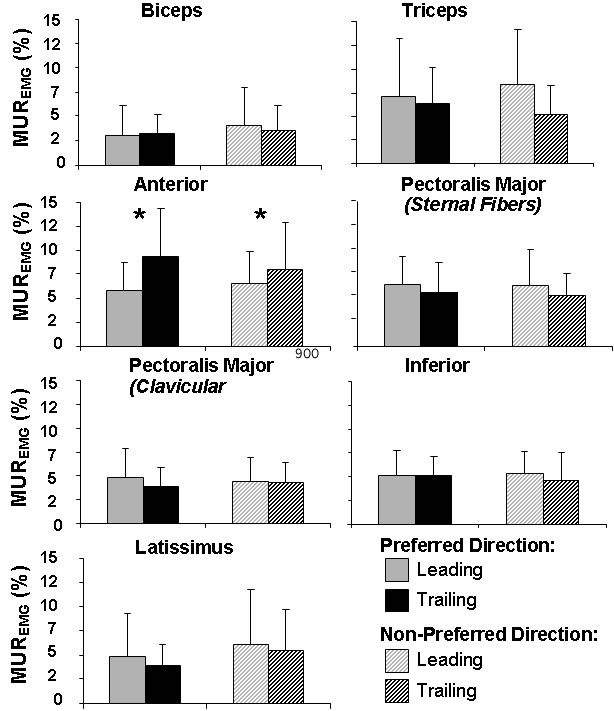
Figure 2. (Click for larger view)
Five of the seven muscles tested had high (MUR>50%) peak values; the sternal fibers of the pectoralis major (both limbs), the trailing U/L of the anterior deltoid, triceps brachii (both limbs), and the leading U/L for the inferior trapezius and latissimus dorsi. The remaining muscles had moderate (MUR 25 to 50%) peak levels (Figure 2). The sternal fibers of the pectoralis major (both limbs), along with the trailing U/L of the anterior deltoid, triceps brachii (both limbs) and leading U/L of the latissimus dorsi had the highest overall muscular demand. The biceps brachii was the least active muscle for both approaches (Figure 3).
DISCUSSION
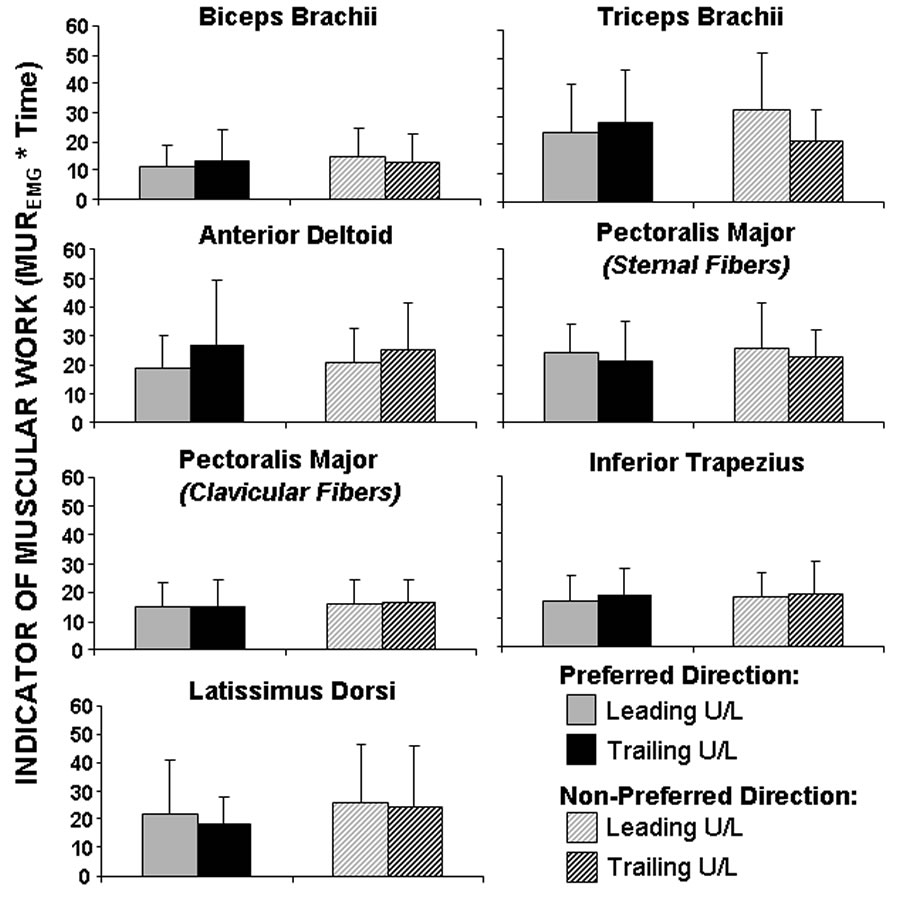
Figure 3. (Click for larger view)
The hypothesis that the muscular demand would be greater during transfers performed from the non-preferred side than the preferred side was not supported in this study. The few significant differences could be accounted for with several reasons. The first of these reasons is, the participants in the study where all highly functional individuals and athletes. In addition to being capable athletes, some participants had the ability to partially stand. This allowed them to semi-stand and pivot during the transfers relieving muscle demand in the U/Ls. The combination of the highly functional athletes recruited as well as the few participants that where able to partially stand may have resulted in a sample non-representative of the manual wheelchair population. Other possibilities for the few significant differences could be the level of difficulty of the transfer. The level height combined with the no gap between the chair and tub bench made the transfer to be among the easiest transfers for an individual to complete. Asking participants to complete a transfer of higher difficulty may have inflated the results found in this study leading to more significant differences.
Consistent with previous studies however, completion of the transfer tasks placed large muscular demands on the U/Ls. Gagnon et al. reported the trailing U/L is responsible for pushing the body away from the initial seat resulting in the abductor muscles being more active5. The anterior fibers of the deltoid, a strong abductor and flexor of the shoulder, showed to have a significantly higher peak muscle demand in the trailing U/E as opposed to the leading U/E. Gagnon et al. also reported the leading U/L is predominantly used for pulling the body towards the target seat resulting in adductor muscles being more active5. Despite the statistically insignificant values, we were able to observe shoulder adductors for the leading U/L to reach a higher peak muscle demand than the trailing U/L with the exception of the clavicular fibers of the pectoralis major during the non-preferred approach. In this test, the leading and trailing U/E had nearly identical peak demand, although a slightly higher overall muscular demand was recorded for the trailing U/E. This could be due to the clavicular fibers of the pectoralis major also playing a role in shoulder flexion which is more prevalent in the trailing U/L when initially lifting the body to assist in supporting the added weight.
The results for the biceps brachii muscle having a 6.06% higher peak muscle demand in the non-preferred approach may play a part in an individual selecting a preferred side. This value multiplied by the number of transfers completed throughout the day could accumulate and lead to a significant increase of fatigue when forced to transfer from the non-preferred side. The latissimus dorsi also was found to have a 13.5% higher peak muscle demand in the non-preferred approach although this was not found to be significant due to the high variability in the muscle.
CONCLUSION
Results of this study shows an individual’s preference to transfer approach is not primarily linked to a muscular advantage, however, they do give us a better understanding of the muscular demand required to complete sitting pivot transfers. The preference may instead be linked to such factors as having the dominant U/L be in the trailing position to support more weight during the lift of the transfer. More research needs to be done to find what factors lead to a preference in transfer approach as well as find a better method of transferring that will limit the high occurrence of injury during transfers.
REFERENCES
- Perry, J., Gronley, J., Newsam, C., Reyes, M., 1996. Electromyographic analysis of the shoulder muscles during depression transfers in subjects with low-level paraplegia. Arch Phys Med Rehabil; 77, 350-355.
- Gagnon, D., Nadeau, S., Noreau, L., Dehail, P., Gravel, D. 2008. Quantification of reaction forces during sitting pivot transfers performed by individuals with spinal cord injury. J Rehabil Med; 40, 468-476.
- Nyland, J., Quigley, P., Huang, C., Lloyd, J., Harrow, J., Nelson, A., 2000. Preserving transfer independence among individuals with spinal cord injury. Spinal Cord; 30, 649-657.
- Forslund, E.B., Granström, A., Levi, R., Westgren, N., Hirschfeld, H., 2007. Transfer from table to wheelchair in men and women with spinal cord injury: coordination of body movement and arm forces. Spinal Cord; 45, 41-48.
- Gagnon, D., Nadeau, S., Noreau, L., Eng, J., Gravel, D., 2008. Trunk and upper extremity kinematics during sitting pivot transfers performed by individuals with spinal cord injury. Clinical Biomechanics; 23 (3), 279-290.
- Butler, H., Newel, R., Hubley-Kozey, C., Kozey, J., 2007. The Interpretation of abdominal wall muscle recruitment strategies change when the electrocardiogram (ECG) is removed from the electromyogram (EMG). J Electromyogr Kinesiol; doi:10.1016/j.jelekin.2007.10.004
ACKNOWLEDGEMENTS
This material is based upon work supported in part by the VA Rehabilitation R&D Service (Projects #A4489R and #B3142C), National Science Foundation (EEC 0552351) and a donation from the Paralyzed Veterans of America.
Author Contact Information:
Eric Brindle, Human Engineering Research Laboratory, VA Pittsburgh Healthcare System, 7180 Highland Dr., Building 4, 252se, Pittsburgh, PA 15206; email: edb12@pitt.edu